A RESEARCHER'S PERSPECTIVE: New Knowledge and New Treatment Possibilities in PTSD and Suicide

A RESEARCHER'S PERSPECTIVE - from Brain & Behavior Magazine, September 2021 issue
By Lynnette A. Averill, Ph.D.
Associate Professor, Baylor College of Medicine Clinical Research Psychologist,
Michael E. DeBakey VA Medical Center
Adjunct Assistant Professor, Yale School of Medicine
National Center for PTSD – Clinical Neurosciences Division,
VA Connecticut, U.S. Department of Veterans Affairs
2015 BBRF Young Investigator
Dr. Lynnette Averill is experienced in translational clinical neuroscience with work focused on informing our understanding of the causes and consequences of trauma-related psychopathology and suicidality, and the investigation of novel rapid-acting interventions. She is interested synaptic connectivity as a biomarker and treatment target, and has special interest in the role that ketamine and psychedelics (including psilocybin, MDMA, and 5-MeO-DMT) can play in biomarker testing due to their rapid effects on synaptic connectivity, behavior, mood, and cognition.
The somewhat blurry pictures on this page are of my father, an enlisted U.S. Marine. One was taken in Vietnam, in his dress blues, and one with his treasured car in rural Montana where he and I both grew up. He and my uncle, his younger brother, served in Vietnam. My uncle died in Vietnam and I sometimes say my father did, too, though he came home fully alive. It wasn’t until the early 1980s when PTSD was included in the DSM—the Diagnostic & Statistical Manual psychiatrists use to make diagnoses. My father, like so many veterans, struggled with what he had experienced in the war and was not able to get answers or effective treatments. Ultimately, he died by suicide when I was 3 years old.
I have no memory of him at all, but I certainly grew up very aware of the effects of war, of stress, and of trauma— not only on the individuals who experienced those things themselves, but also the families, the friends, the communities, who, to a degree, experienced them in parallel and all too often end up losing loved ones to suicide.
Throughout my career as a researcher and clinician, I’ve asked: how can we effectively treat stress and traumarelated symptoms? How do we effectively treat suicidal ideation, specifically? I found a quote that I really like. It says, “Reality is the leading cause of stress among those in touch with it.” It may seem silly. But I think it gets at the idea that reality, while beautiful and wonderful in so many ways, is also filled with stress and trauma. For the majority of the population, life will include trauma, sometimes in a single moment or event, and sometimes in chronic and persistent ways across days, months, or decades. Further, the experience of living day-to-day with PTSD, depression, suicidal thoughts, and related things are, in and of themselves, chronic stressors.
Suicidality, which includes suicidal thoughts and behaviors, is often related to stress and trauma. Right now, there isn’t a formal diagnostic category for suicidal thoughts and behaviors in the DSM, although it has been proposed and is currently being considered for inclusion in the next addition.
We have a suicide epidemic in this country and also globally. Worldwide, we lose one person to suicide about every 40 seconds, which is a truly staggering number. Here in the U.S. it’s approximately 130 people a day, of whom about 20 are veterans.
In view of these numbers, there’s no debate and no question that we need to be doing something different, something more. This is what my career has been focused on: how we can improve treatments and outcomes. With support from the Brain & Behavior Research Foundation, the American Foundation for Suicide Prevention, the Department of Veterans Affairs, and some other groups, my research has been looking not only at the clinical and behavioral factors of risk and resilience related to PTSD and suicidality, but also at the neurobiological underpinnings.
NEURAL FINGERPRINTS
It’s been pointed out that mental illness has such a stigma in part because it’s possible to look at an individual and say, “Well, I don’t see anything immediately wrong with you. You don’t have a cast, you don’t have bandages. I don’t see anything wrong—so there must not be anything wrong.”
But we know from decades of neuroscience research that this really is not the case. There are “invisible injuries,” neurobiological changes, that occur. Another quote I often share is by the writer Laurell Hamilton: “There are wounds that never show on the body, that are deeper and more hurtful than anything that bleeds…” Within stress and trauma, there are three primary brain regions that have been implicated: the prefrontal cortex, amygdala, and hippocampus. Over and over again we have seen evidence that these parts of the brain are significantly affected in various ways related to stress and trauma.
What does suicidal ideation or suicide attempts look like in the brain? Is there some sort of biological fingerprint that we can identify? We have some preliminary data that certain areas in the brain have significant changes in cortical thickness, which is used in this case as a measure of brain health, and can be affected, for instance, by injury or insult to the brain.
We have studied a sample of veterans with PTSD, some of whom reported they had thought of suicide and some who had never had such thoughts. Our data shows that there may be something unique, structurally, in the brains of individuals who report an experience of suicidal ideation. This data is very preliminary right now, and we’re actively enrolling and recruiting additional participants who will add to this data set, as well as collecting much richer data around the experiences of suicidality.
In addition to brain structure we are also looking at connectivity, which tells us about brain function. Our attention is drawn to three networks. First, the salience network, which is kind of an alarm system that tells us what things we need to be paying attention to. Sometimes those are mundane things, sometimes they are potential threats or dangers. Second, the central executive network, which involves top-down regulation of emotion, decision-making, and planning. Third is the default mode network, the part of our brain that is most active when we are at rest, from a cognitive perspective.
The data shows that there are perhaps unique neural fingerprints, a neural signature in connectivity in veterans with suicidal ideation and behavior. The question is what we can do with this knowledge, presuming we are able to confirm it and learn more about it.
A NEW TREATMENT FRONTIER?
We know that traditionally available treatments quite rarely even scratch the surface of suicidal ideation for a lot of individuals, which of course is very concerning. It’s said that the definition of insanity is doing the same thing over and over and expecting different results. If you want different results, at some point you have to try different approaches.
Over the last 5 to 10 years there has been an explosion in different approaches, which I think is really exciting. My perspective is that we’re on the forefront of a new frontier in terms of psychiatric medicines that we might use to treat people with suicidal ideation and behavior. One is ketamine. There is also the possibility that psychedelic medicines may be useful.
Ketamine is a drug that we have done a lot of work with. It is really exciting in that it works in the brain in a way that is completely different from SSRIs, the serotonin reuptake inhibitor drugs usually used to treat depression. Ketamine has been shown to work rapidly in individuals with severe depression who have not found relief in standard antidepression therapies.
We have been able to give ketamine to individuals who are struggling with depression, PTSD, and suicidality, and generally within 24 hours they’re feeling remarkably better, have a significant improvement in symptoms.
I want to note that SSRIs are incredibly important drugs and for the people that they work well for—they are literally lifesaving. The problem is that for a lot of people they don’t work well. That’s why we’re exploring what other things we can put into our toolkit.
We’ve been able to use MRI imaging and other sorts of tools to look at how ketamine is working, as well as how those changes in the brain seem to relate to changes in symptoms. Much of this seems to involve changes in synaptic strength— changes in the strength of connections between neurons, which we call plasticity. This may provide a biological target that will enable us to develop other treatments with the potential to improve and ultimately save lives.
I say other treatments with the same potential to help because ketamine is a dissociative anesthetic. That means people who take it can have dissociative experiences—people will talk about feeling that their thoughts are a bit jumbled or that they feel as if they are floating, disconnected from their body. Sometimes, people have visual or auditory hallucinations. In our experience with ketamine, side effects have been well tolerated and brief in duration, since ketamine has a short half-life in the body, lasting only minutes.
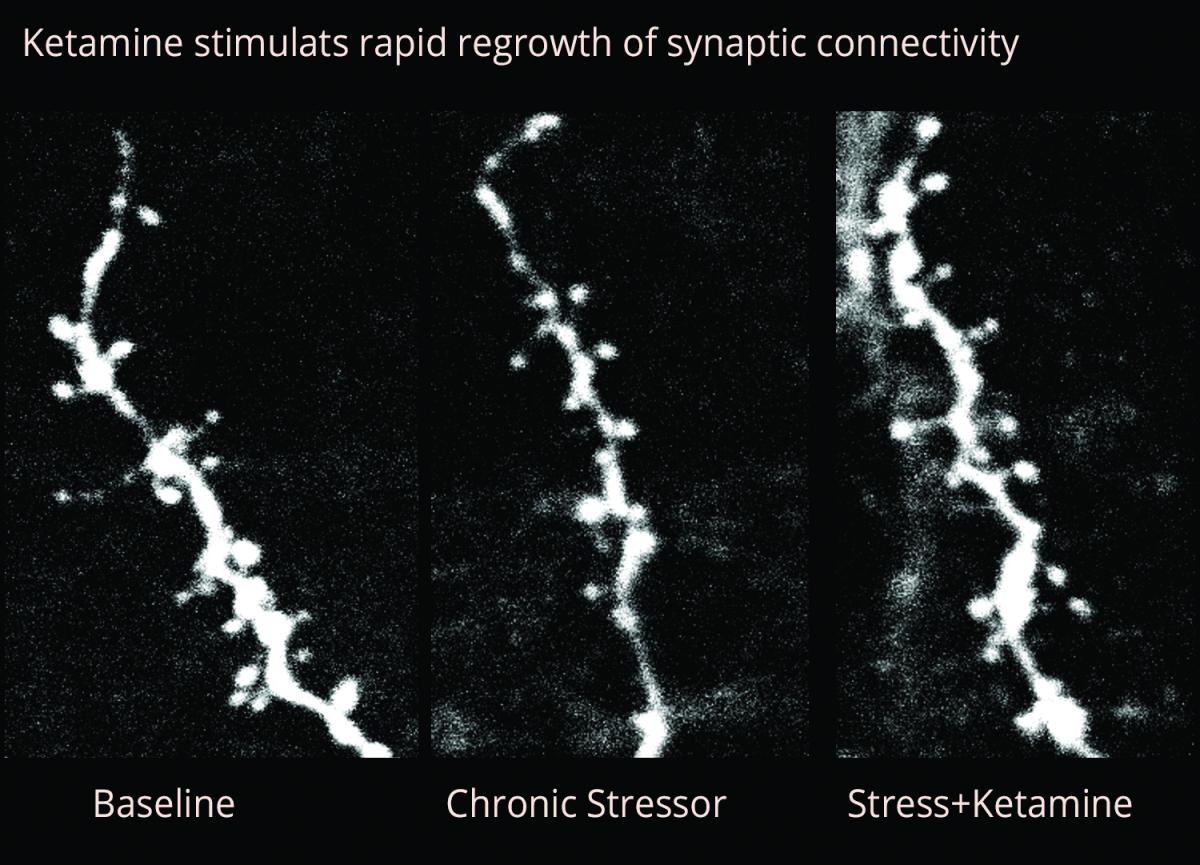
This image immediately shows a dendrite in the mouse brain with little features called spines protruding from it. These are the points at which connections are made with other neurons. The image at LEFT is “baseline,” i.e., before we subject the animal to stress. You can see the dendrite is pretty plumped up and there are a lot of spines on it. The MIDDLE image shows what happens when there is exposure to a chronic stressor. When there’s stress, it kind of shrinks down, and some of those spines go away. Then, in the RIGHT image, you see what happens after we give ketamine following exposure to a stressor. You can see that the dendrite really plumps up again, which corresponds with increases in synaptic strength and synaptic density. The number of spines and dendrites has really expanded again.
{kind=link}
That is incredibly positive, not only from a behavioral perspective, but also from a cognitive and symptoms perspective. Other research we’ve done tells us that within 24 hours of a ketamine infusion, abnormal connectivity in the brain in people with depression has shifted, and very closely resembles connectivity in the brain of unaffected, un-depressed individuals. I call your attention to this in order to suggest that not only does ketamine work rapidly to relieve symptoms; it also works rapidly to change underlying neurobiology.
One of the potential drawbacks of ketamine is the short durability of its therapeutic effect. The response typically lasts a maximum of 10 days to 2 weeks. I was part of a large team based at Yale— it included many BBRF grantees—which last year demonstrated that pre-dosing individuals with the immunosuppressant drug rapamycin extended the therapeutic effects of ketamine in people who were depressed, in some cases for several additional weeks.
Recently we’ve gone back to that data and specifically looked at the individuals who reported suicidal ideation. Interestingly, we found that the trajectory of recovery and relapse for suicidal ideation is not at all the same as it is for depression symptoms generally. This suggests, perhaps not surprisingly, that suicidality is not simply a sub-symptom of depression, but is something unique, neurobiologically.
To be clear: suicidal ideation generally improved across the board, but it did have a very different trajectory than did symptom improvement in individuals with depression. This is leading us now to look for fingerprints in those connectivity networks I mentioned earlier—an approach we call “connectome fingerprinting.” This means analyzing the connectivity profiles of individuals with PTSD and suicidality who respond to ketamine, and who don’t respond to ketamine. We hope to compare their profiles with those of depressed people who do and don’t respond to ketamine.
POTENTIAL OF PSYCHEDELICS
I also want to mention possible applications of psychedelic medicines and especially what we call psychedelicassisted psychotherapy. Current research is conducted under what’s called the medical model for these substances. You go to a hospital, are given the dosing by a qualified medical team, and you have trained mental health professionals to manage the psychotherapy portion of the treatment. This is called psychedelicassisted psychotherapy.
Psychedelic medicines are not a new thing, but in the last 5 to 10 years there has been a rebirth of interest in performing new research on their potential use in a variety of psychiatric illnesses, including severe depression, PTSD, and suicidality.
I have a collaboration with an investigator at Yale. We’re looking at anti-suicidal effects of MDMA. This is a psychedelic drug that in its illegal street form is called Ecstasy. Like our experiments with ketamine in depression, our experiments with MDMA involve its use in highly controlled situations and dosages. We will also be looking at possible antisuicidal effects of psilocybin, another psychedelic. Both MDMA and psilocybin have side effects in some people that include anxiety and increase in heart rate and blood pressure. This is why it’s crucial to give these substances in an appropriate setting and under the guidance of highly trained professionals.
In July 2020, Alan Davis and I published a study in the journal Chronic Stress that looked at psychedelics specifically in Special Operations Forces veterans. These are the elite of our military personnel. They are selected for Special Forces because they have demonstrated not only exceptional physical strength, but also exceptional emotional and cognitive strength. Many have had considerable trauma exposure. The population that we had in our study averaged over 10 deployments each, some as many as 18, which is remarkable.
In this population, as with all veterans, but perhaps even more so, there’s a great deal of stigma around mental illness, a great deal of stigma around admitting that they are struggling. They may have unexpressed concerns about PTSD and suicidality, and there are very high rates of suicide among them, unfortunately.
The Special Forces veterans in our analysis, nearly all of whom were Iraq/ Afghanistan veterans, had completed a psychedelic clinical program in Mexico between 2017 and 2019. We asked them to recall, retrospectively, their mental health and cognitive functioning during the 30 days before and 30 days after treatment two plantbased psychedelics (ibogaine and 5-MeO-DMT).
Our study sample comprised 51 Special Forces veterans suffering from psychological and cognitive impairment. Results suggested that ibogaine and 5-MeO-DMT may offer a rapid and robust, and well-tolerated, treatment option for those suffering from a variety of psychiatric and cognitive symptoms. However, we noted that further research is needed to support this preliminary evidence, specifically, randomized, double blind, placebo-controlled trials to determine the safety and efficacy of these two substances. I should also note that our study did not assess any adverse effects or side effects.
I want to highlight significant changes in suicidal ideation, as well as in general mental health symptoms, that these and other veterans treated with psychedelic substances have reported. In the study I have just referred to, results indicated significant and very large reductions in retrospective report of suicidal ideation, as well as cognitive impairment and symptoms of PTSD. Some of this improvement may have been associated with increased psychological flexibility.
Most of the participants rated the psychedelic experiences as one of the top five personally meaningful (84%), spiritually significant (88%), and psychologically insightful (86%) experiences of their lives, which impressed us. We are preparing to evaluate prospective and longitudinal data from this same clinic.
We will be doing a study specifically looking at suicide in people with treatment-resistant PTSD and suicidal ideation. We hope to obtain connectome fingerprints, as we did in our ketamine research in depressed patients. We want to look for differences between those who seem to respond and those who do not, with an eye to using this knowledge to inform precision-medicine efforts. The idea is to take that kind of information and develop compounds that can target those same aspects of the brain, but with a different side-effect profile.
Right now, about 130 Americans are dying each day by suicide, including 20 or more veterans. Broadly speaking, I think the thing that’s exciting about ketamine and psychedelic medicines is that if we can increase the number of approaches we have in our toolbox and improve our ability to know who might be the best candidates for which treatments, this will allow us to not only save lives, but to help people build lives they truly want to live.
Click here to read the Brain & Behavior Magazine's September 2021 issue